العربية
العربية
 Français
Français
 Português
Português
 Русский
Русский
 Español
Español
 Uzbek
Uzbek
 Myanmar
Myanmar
Description:
Cardiac arrest is a medical emergency with high global morbidity and mortality rates, closely linked to the growing burden of cardiovascular diseases. This article analyzes the epidemiology of cardiac arrest and presents treatment strategies following the “chain of survival,” including high-quality cardiopulmonary resuscitation (CPR), early defibrillation, emergency medications, and post-resuscitation care to improve survival outcomes.
Main Content
Cardiac arrest is a sudden cessation of heart function, leading to a loss of blood circulation and oxygen supply to vital organs, particularly the brain. It is a critical medical emergency and often results in death if not promptly treated. Cardiac arrest can occur out-of-hospital (OHCA) or in-hospital (IHCA) and is a leading cause of sudden cardiac death (SCD) (1).
According to the World Health Organization (WHO), cardiovascular diseases (CVDs) are the leading cause of death globally, accounting for approximately 17.9 million deaths annually, over 80% of which are due to heart attacks and strokes (1). Cardiac arrest significantly contributes to this, estimated to account for 15–20% of all deaths (2).
Global Epidemiology of Cardiac Arrest
Cardiac arrest represents a major public health issue, with incidence varying by region and healthcare system. According to the American Heart Association (AHA) 2025 report, the global incidence of adult OHCA is estimated at 55–81 cases per 100,000 population per year (3), translating to millions of cases annually. For example, in the United States, there are over 356,000 OHCA cases each year—nearly 1,000 per day—with approximately 90% mortality (4). Globally, cardiac arrest causes more deaths than colorectal cancer, breast cancer, prostate cancer, influenza, pneumonia, car accidents, HIV, gun violence, and house fires combined (5).
Survival rates after OHCA remain low—only around 8–10% survive to hospital discharge. Recent analyses show that rates of return of spontaneous circulation (ROSC) are approximately 29.7%, survival to hospital admission 22%, survival to discharge 8.8%, 1-month survival 10.7%, and 1-year survival 7.7% among OHCA patients who receive CPR (7). These figures highlight significant disparities between developed and developing countries, where emergency medical services (EMS) are often uneven.
Regarding sudden cardiac death (SCD), it accounts for 20% of all deaths in Western societies and about 50% of global cardiovascular deaths. Globally, SCD is increasing among younger adults (ages 25–44), with SCD-related mortality rising in the U.S. over the past two decades, along with racial and regional disparities (8). In the U.S., approximately 436,000 deaths occur annually due to cardiac arrest (5).

Source image: https://www.sca-aware.org/about-sudden-cardiac-arrest/latest-statistics
Demographics and Risk Factors
Cardiac arrest is more common in males than females, with the highest incidence in those over age 65 (over 50%) (9). In the U.S., bystander-witnessed OHCA accounts for 37.1%, EMS-witnessed 12.8%, and unwitnessed cases 50.1%. In children, the annual OHCA incidence is lower, estimated at 7,000–23,000 cases, primarily occurring at home (87.5%) (10). Research shows pediatric OHCA has a ~90% mortality rate, similar to adults, with notable racial disparities observed among young athletes (11).
Major risk factors include underlying cardiovascular disease (e.g., coronary artery disease), hypertension, diabetes, obesity, smoking, and a sedentary lifestyle. Air pollution and environmental factors also contribute. During the COVID-19 pandemic, OHCA rates tripled in some areas, with delayed CPR and reduced survival (12). Racial disparities persist, with Hispanic, Black, and Asian individuals having lower survival rates compared to White patients (11).
For IHCA, incidence varies by country and is generally higher in developing nations due to limited resources. While IHCA mortality has declined, it remains high (13).
Future Trends in Cardiac Arrest Incidence
The global incidence of cardiac arrest is projected to continue rising, driven by increasing life expectancy, growing rates of cardiovascular disease, diabetes, and obesity. In low- and middle-income countries, the burden may be exacerbated by weaker healthcare systems, limited access to AEDs (Automated External Defibrillators), and inadequate CPR training. In developed nations, population aging also contributes to the growing cardiac arrest risk, posing a major challenge for emergency care and prevention globally (16).
Strategies for Treatment and Prevention
Treatment strategies follow the “Chain of Survival”, including early recognition, emergency response, CPR, defibrillation, and post-resuscitation care (14). High-quality CPR combined with early defibrillation significantly increases survival, especially in cases of ventricular fibrillation. Epinephrine 1 mg IV every 3–5 minutes is recommended for non-shockable rhythms, along with addressing underlying causes like pulmonary embolism or myocardial infarction (15). After ROSC, patients require intensive care, targeted temperature management, and multidisciplinary rehabilitation. Prevention efforts emphasize a healthy lifestyle, community CPR training, and public access to AEDs (11).
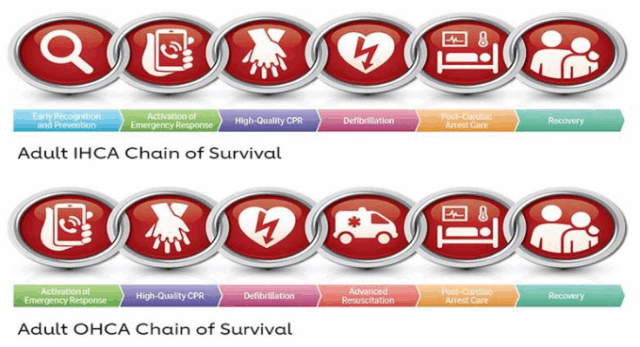
Figure 2. 2020 American Heart Association Chains of Survival for IHCA and OHCA
CPR: cardiopulmonary resuscitation; IHCA: in-hospital cardiac arrest; OHCA: out-of-hospital cardiac arrest.
Conclusion
Cardiac arrest represents a global burden with high incidence and low survival rates, especially in low-resource settings. Improving EMS systems, enhancing public education, and adherence to evidence-based guidelines are essential to reduce mortality.
To support optimal cardiac arrest management, Vinphaco offers high-quality injectable products, including:
- ADRENALINE – Vitapure (Adrenaline 1mg/10ml)
- ADRENALIN (Adrenaline tartrate 1.82mg/ml)
These vasopressor medications contain adrenaline (epinephrine)—a key active ingredient recommended in international cardiac arrest resuscitation guidelines.
References: